Overview

Fallen arches, flat feet, or Plantar fasciitis can cause pain and discomfort in the legs, feet, ankles, Achilles tendon, hips, and low back. In this video, Ron Vaughn, a sports massage therapist, and Christie Powell, a physical therapist, explain how the feet become pronated (fallen arches) and how some simple at-home exercises can strengthen the arch muscles to allevaite pain and discomfort.
Causes
As children grow, their legs will experience developmental changes that can result in excess flattening of the arches with weight bearing. One example is genu valgum, or knock-knees, a usually normal, temporary condition in children at different stages of growth. A tight calf muscle or Achilles tendon can also contribute to a flat foot. Many children will experience tight calf muscles as they go through growth spurts. Conditions that are present at birth and are often diagnosed early include: metatarsus adductus, calcaneovalgus and congenital vertical talus. Tarsal coalitions are congenitally fused foot bones that cause a rigid flat foot often associated with painful muscle spasms. This type of flat foot is usually diagnosed later in childhood or in adulthood. Any condition that causes loose ligaments can result in a flat foot or lower-than-normal arch. Ligaments are bands of tissue that connect bones to each other and have an important role in giving form to foot arches. An example of a condition that causes loosening of ligaments is pregnancy, where normal hormonal changes relax the ligaments. Diseases that cause loose ligaments include Ehlers-Danlos syndrome, Marfan's syndrome and rheumatoid arthritis. If one leg is longer than the other, one foot may be flat in relation to the other to compensate. Usually the foot on the longer limb will have a flatter arch in an effort to shorten that limb, balancing-out the unevenness. Leg length inequality can be caused by spinal abnormalities such as scoliosis. It can also be due to an actual difference in length of one leg bone compared to the other.
Symptoms
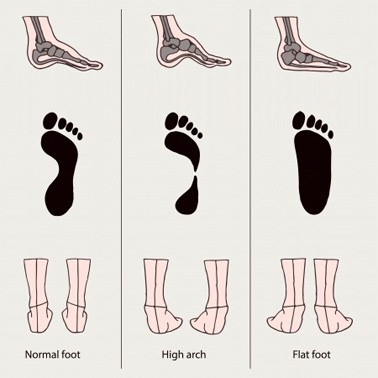
It?s possible to have fallen arches and experience no symptoms whatsoever. But many people do notice some problems with this condition. Their feet, back and legs ache. Standing on their toes is difficult, if not impossible, and they note swelling around the arch and heel.
Diagnosis
An examination of the foot is enough for the health care provider to diagnose flat foot. However, the cause must be determined. If an arch develops when the patient stands on his or her toes, the flat foot is called flexible and no treatment or further work-up is necessary. If there is pain associated with the foot or if the arch does not develop with toe-standing, x-rays are necessary. If a tarsal coalition is suspected, a CT scan is often ordered. If a posterior tibial tendon injury is suspected, your health care provider may recommend an MRI.
Is flat footedness genetic?
Non Surgical Treatment
Most cases of fallen arches are not painful and need no form of treatment. However, common symptoms of fallen arches can include pain in your feet (particularly in the area of your heel or arch), pain in your feet that persists after long bouts of physical activity or standing up, achy feet, or arch pain when standing on the tips of your toes. Most cases of fallen arches are not preventable. Treatments for fallen arches include, rest, ice, compression, medication to relieve pain, orthotics, or in some cases surgery.
Surgical Treatment

A better approach is to strengthen the weakened ligaments with Prolotherapy, supplemented by an arch support if the condition has existed for several years. Chronic pain is most commonly due to tendon and ligament weakness, or cartilage deterioration. The safest and most effective natural medicine treatment for repairing tendon, ligament and cartilage damage is Prolotherapy. In simple terms, Prolotherapy stimulates the body to repair painful areas. It does so by inducing a mild inflammatory reaction in the weakened ligaments and cartilage. Since the body heals by inflammation, Prolotherapy stimulates healing. Prolotherapy offers the most curative results in treating chronic pain. It effectively eliminates pain because it attacks the source: the fibro-osseous junction, an area rich in sensory nerves. What?s more, the tissue strengthening and pain relief stimulated by Prolotherapy is permanent.
Fallen arches, flat feet, or Plantar fasciitis can cause pain and discomfort in the legs, feet, ankles, Achilles tendon, hips, and low back. In this video, Ron Vaughn, a sports massage therapist, and Christie Powell, a physical therapist, explain how the feet become pronated (fallen arches) and how some simple at-home exercises can strengthen the arch muscles to allevaite pain and discomfort.
Causes
As children grow, their legs will experience developmental changes that can result in excess flattening of the arches with weight bearing. One example is genu valgum, or knock-knees, a usually normal, temporary condition in children at different stages of growth. A tight calf muscle or Achilles tendon can also contribute to a flat foot. Many children will experience tight calf muscles as they go through growth spurts. Conditions that are present at birth and are often diagnosed early include: metatarsus adductus, calcaneovalgus and congenital vertical talus. Tarsal coalitions are congenitally fused foot bones that cause a rigid flat foot often associated with painful muscle spasms. This type of flat foot is usually diagnosed later in childhood or in adulthood. Any condition that causes loose ligaments can result in a flat foot or lower-than-normal arch. Ligaments are bands of tissue that connect bones to each other and have an important role in giving form to foot arches. An example of a condition that causes loosening of ligaments is pregnancy, where normal hormonal changes relax the ligaments. Diseases that cause loose ligaments include Ehlers-Danlos syndrome, Marfan's syndrome and rheumatoid arthritis. If one leg is longer than the other, one foot may be flat in relation to the other to compensate. Usually the foot on the longer limb will have a flatter arch in an effort to shorten that limb, balancing-out the unevenness. Leg length inequality can be caused by spinal abnormalities such as scoliosis. It can also be due to an actual difference in length of one leg bone compared to the other.
Symptoms
It?s possible to have fallen arches and experience no symptoms whatsoever. But many people do notice some problems with this condition. Their feet, back and legs ache. Standing on their toes is difficult, if not impossible, and they note swelling around the arch and heel.
Diagnosis
An examination of the foot is enough for the health care provider to diagnose flat foot. However, the cause must be determined. If an arch develops when the patient stands on his or her toes, the flat foot is called flexible and no treatment or further work-up is necessary. If there is pain associated with the foot or if the arch does not develop with toe-standing, x-rays are necessary. If a tarsal coalition is suspected, a CT scan is often ordered. If a posterior tibial tendon injury is suspected, your health care provider may recommend an MRI.
Is flat footedness genetic?
Non Surgical Treatment
Most cases of fallen arches are not painful and need no form of treatment. However, common symptoms of fallen arches can include pain in your feet (particularly in the area of your heel or arch), pain in your feet that persists after long bouts of physical activity or standing up, achy feet, or arch pain when standing on the tips of your toes. Most cases of fallen arches are not preventable. Treatments for fallen arches include, rest, ice, compression, medication to relieve pain, orthotics, or in some cases surgery.
Surgical Treatment
A better approach is to strengthen the weakened ligaments with Prolotherapy, supplemented by an arch support if the condition has existed for several years. Chronic pain is most commonly due to tendon and ligament weakness, or cartilage deterioration. The safest and most effective natural medicine treatment for repairing tendon, ligament and cartilage damage is Prolotherapy. In simple terms, Prolotherapy stimulates the body to repair painful areas. It does so by inducing a mild inflammatory reaction in the weakened ligaments and cartilage. Since the body heals by inflammation, Prolotherapy stimulates healing. Prolotherapy offers the most curative results in treating chronic pain. It effectively eliminates pain because it attacks the source: the fibro-osseous junction, an area rich in sensory nerves. What?s more, the tissue strengthening and pain relief stimulated by Prolotherapy is permanent.




 Morton neuromas are focal areas of symptomatic perineural fibrosis around a plantar digital nerve of the foot. The abnormality is non-neoplastic and does not represent a true neuroma. It may more correctly be known as Morton?s metatarsalgia. The condition is thought to be due to chronic entrapment of the nerve by the intermetatarsal ligament. It most often occurs in middle-aged individuals and is many times more common in women than men. Approximately 30% of asymptomatic middle-aged persons have the radiological pathologic findings of a Morton?s neuroma.
Morton neuromas are focal areas of symptomatic perineural fibrosis around a plantar digital nerve of the foot. The abnormality is non-neoplastic and does not represent a true neuroma. It may more correctly be known as Morton?s metatarsalgia. The condition is thought to be due to chronic entrapment of the nerve by the intermetatarsal ligament. It most often occurs in middle-aged individuals and is many times more common in women than men. Approximately 30% of asymptomatic middle-aged persons have the radiological pathologic findings of a Morton?s neuroma.
 Overview
Overview Symptoms
Symptoms